Improving queuing and triage practices is essential for early assessment of medical severity and timely intervention. This study aimed to evaluate the current triaging and queuing processes of Elephant's affiliate healthcare facilities and provide research-based recommendations for designing a triage feature for the Elephant OS.
ROLE
UX Research Lead
RESEARCH CATEGORY
Explorative/ Evaluative research
TOOLS
Miro, Slab, Figma

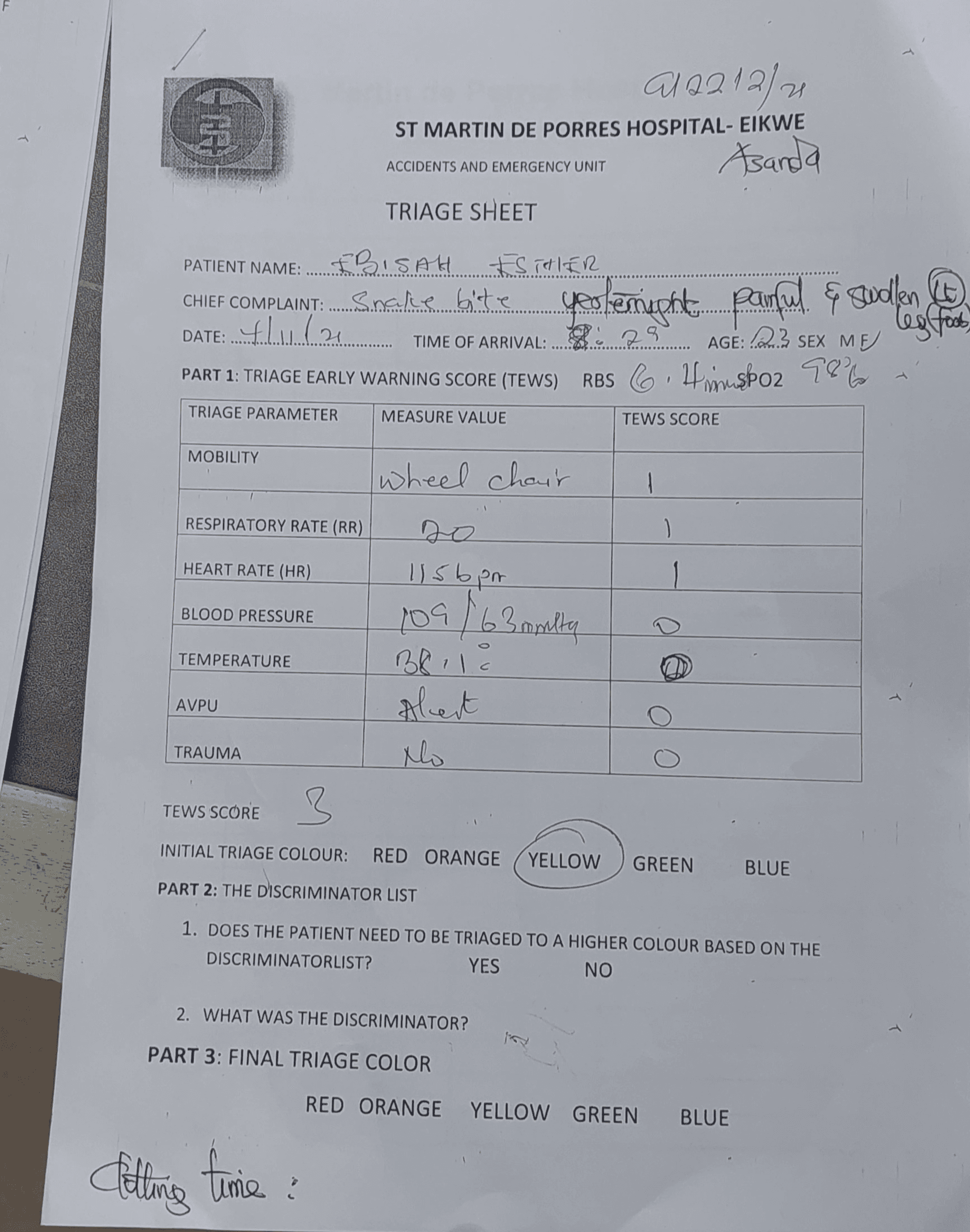
Elephant’s affiliate facilities in Ghana had long relied on a paper-based triage system. This led to poor prioritization and critical communication gaps. Urgent cases were often mismanaged or misclassified, with patients face long wait times for essential care.
Our main objective was to understand the current paper-based triage system, identify its strengths and weaknesses, and adapt it to a digital format that accommodates local healthcare practices.
Research Goals

Desk Research
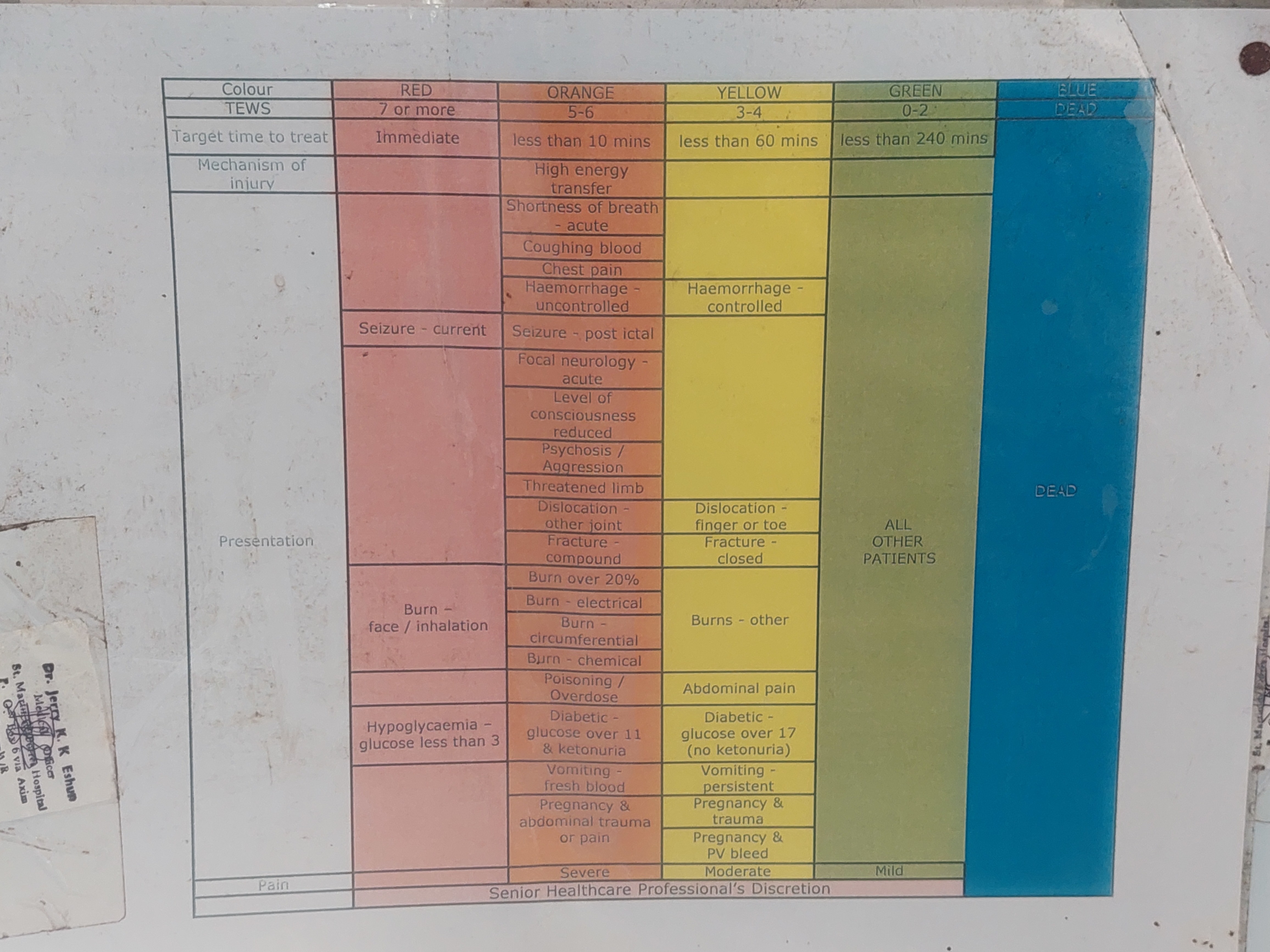
We began by reviewing the African triaging standard, i.e. The South African Triage Scale(SATS). This helped us establish a conceptual understanding of this triage model and how it is used in urgent care intervention.
Conceptual Inquiry
Field visits to Accident and Emergency units in seven healthcare facilities across Ghana’s Western, Ashanti, and Northern regions revealed the triage process in action.
Our observations and follow-up interviews highlighted the patient-health worker dynamic and the flow of information among clinical staff, along with challenges in patient prioritization and structural inefficiencies, further emphasising the need for a streamlined digital solution.
Competitor Analysis
By evaluating triage features of some notable EHR systems on the market Ghanaian market, like OASIS, HAMS, and Lightwave, we were able to identify and analyse strengths and weaknesses in how they integrated triage workflows. Criteria such as user experience, layout, navigation structure, accessibility, and performance were critical in our analysis
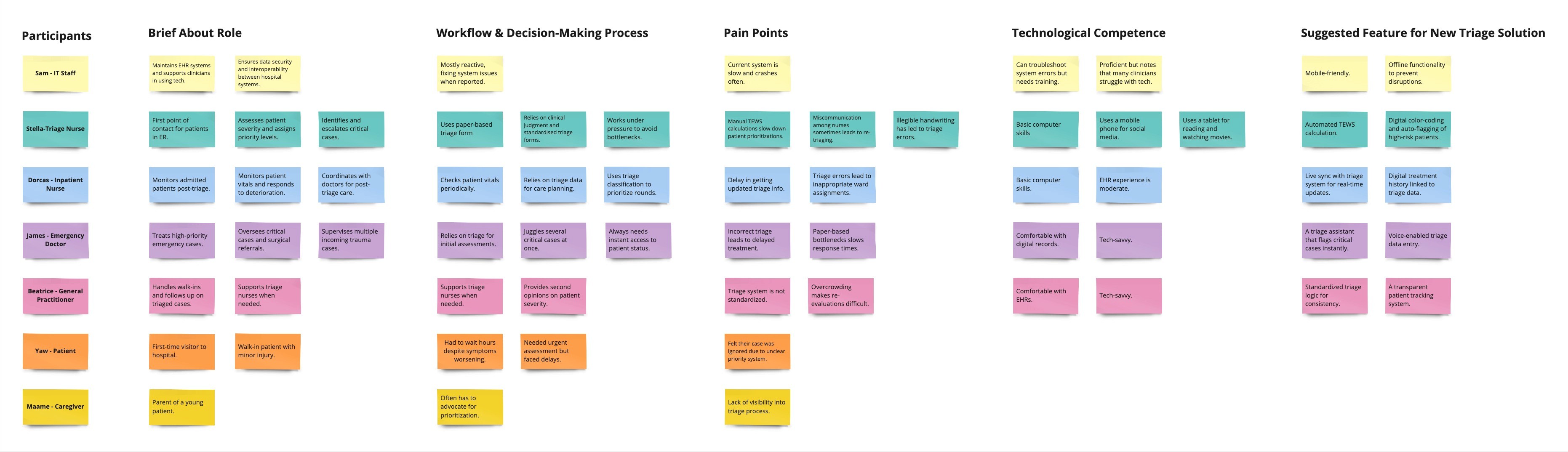
Paper-based bottlenecks
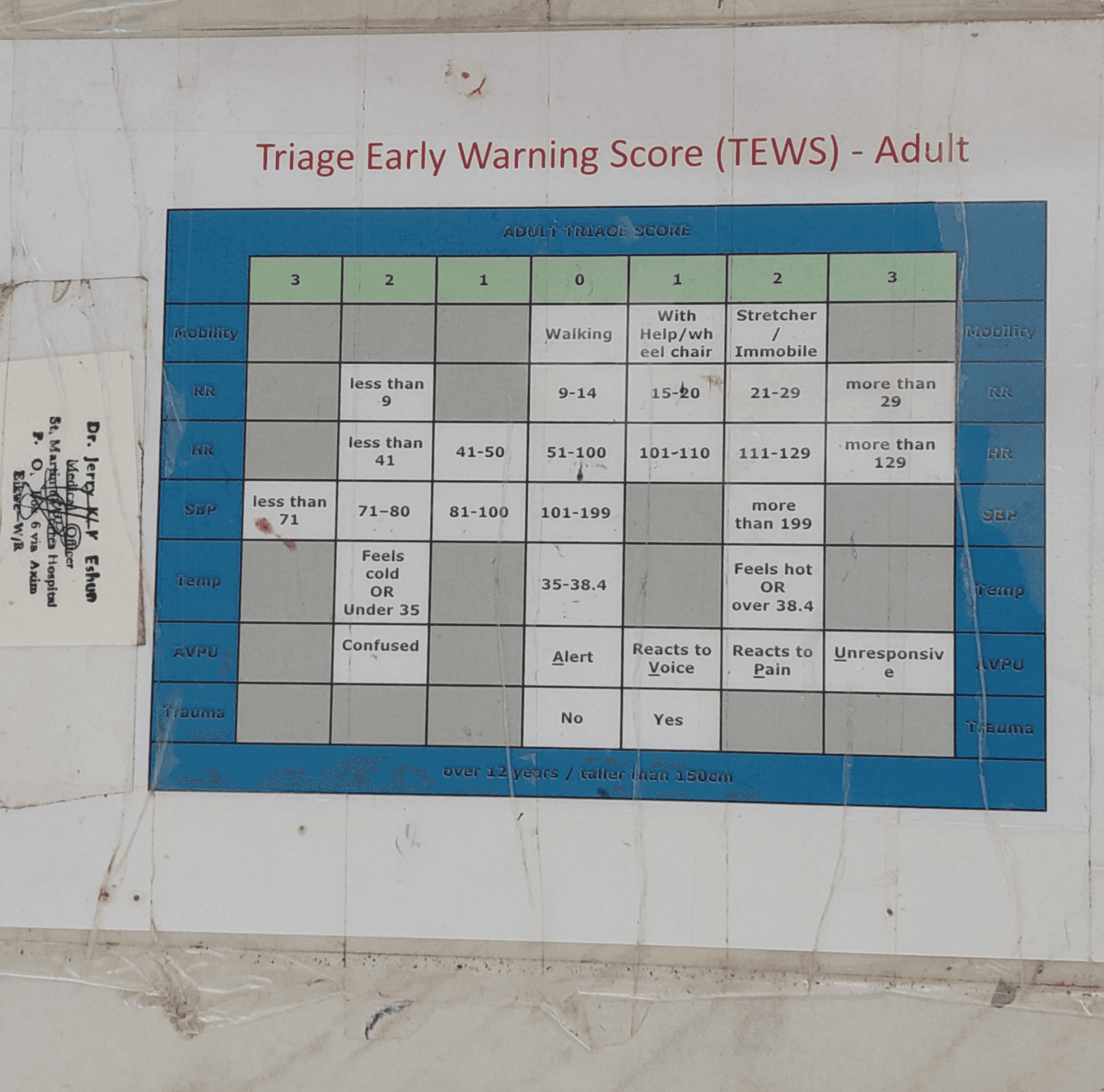
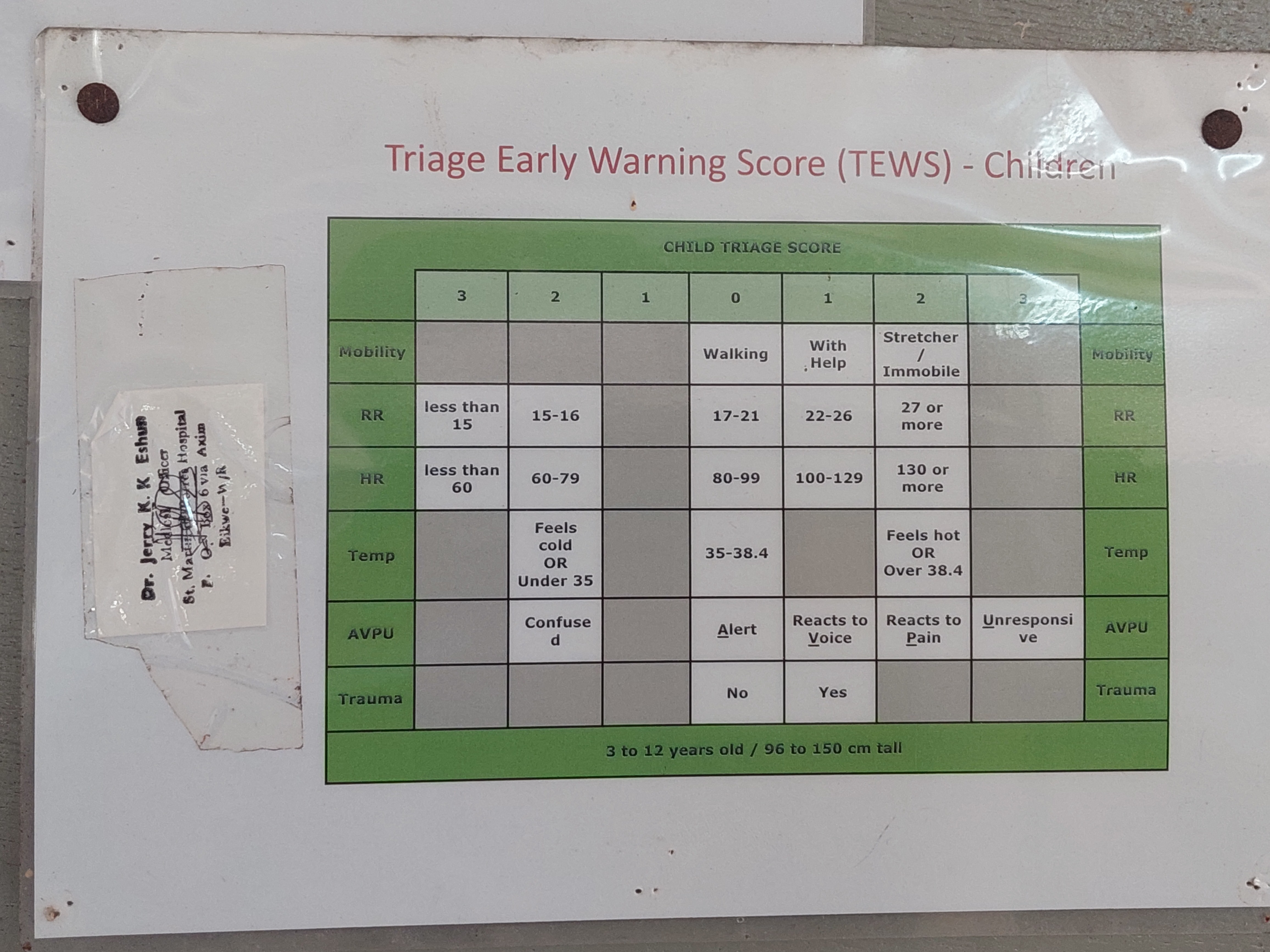
Clinicians rely on outdated paper triage, which prevents consistent patient prioritization. In high-stress settings, urgent cases risk getting overlooked due to small clerical errors. Manually calculating the Triage Early Warning Score (TEWS) consumes critical time and focus needed for patient assessment, a challenge faced by many nurses.
Inconsistent protocols
Inconsistent protocols across facilities caused treatment delays and varied patient experiences. Triage was often subjective, relying on ad hoc verbal assessments instead of standardized forms. This inconsistent prioritization delayed high-risk patients.
For example, I was told of a scenario where communication breakdown once misclassified an acute appendicitis patient as non-urgent, leading to a delay in surgery.
Technological Gaps in Competitor EHRs.
Competitor EHR systems lacked intuitive triage features and were often not optimised for real-world, high-stress scenarios. They mostly lacked automated prioritizations and were unresponsive or available on mobile devices, making them physically impractical for clinicians on the move during patient examinations.
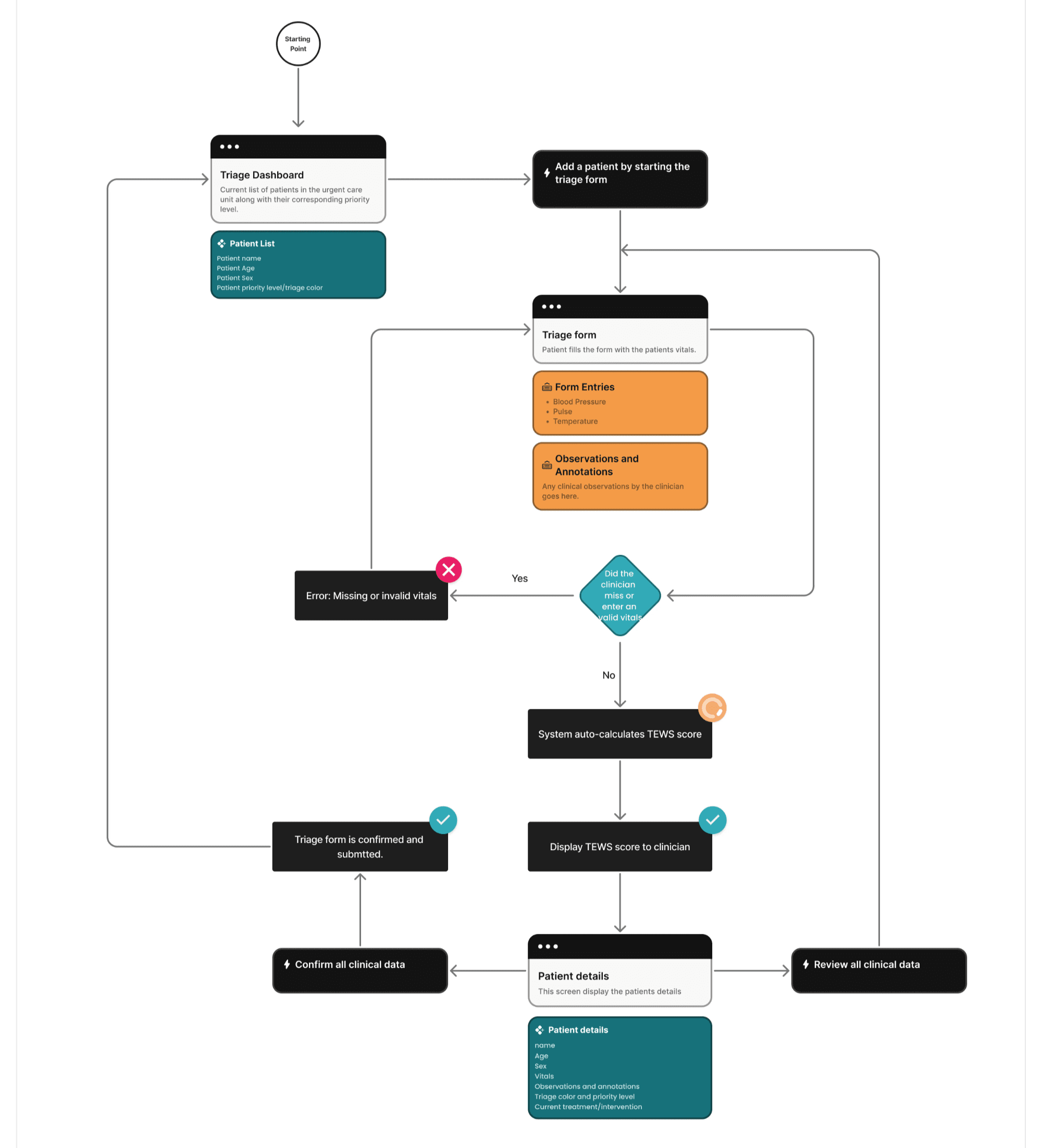
User Flow
Based on our insights we create a high-level user flow of how the patient queuing and triage feature is supposed to function.
Clinicians
Patients
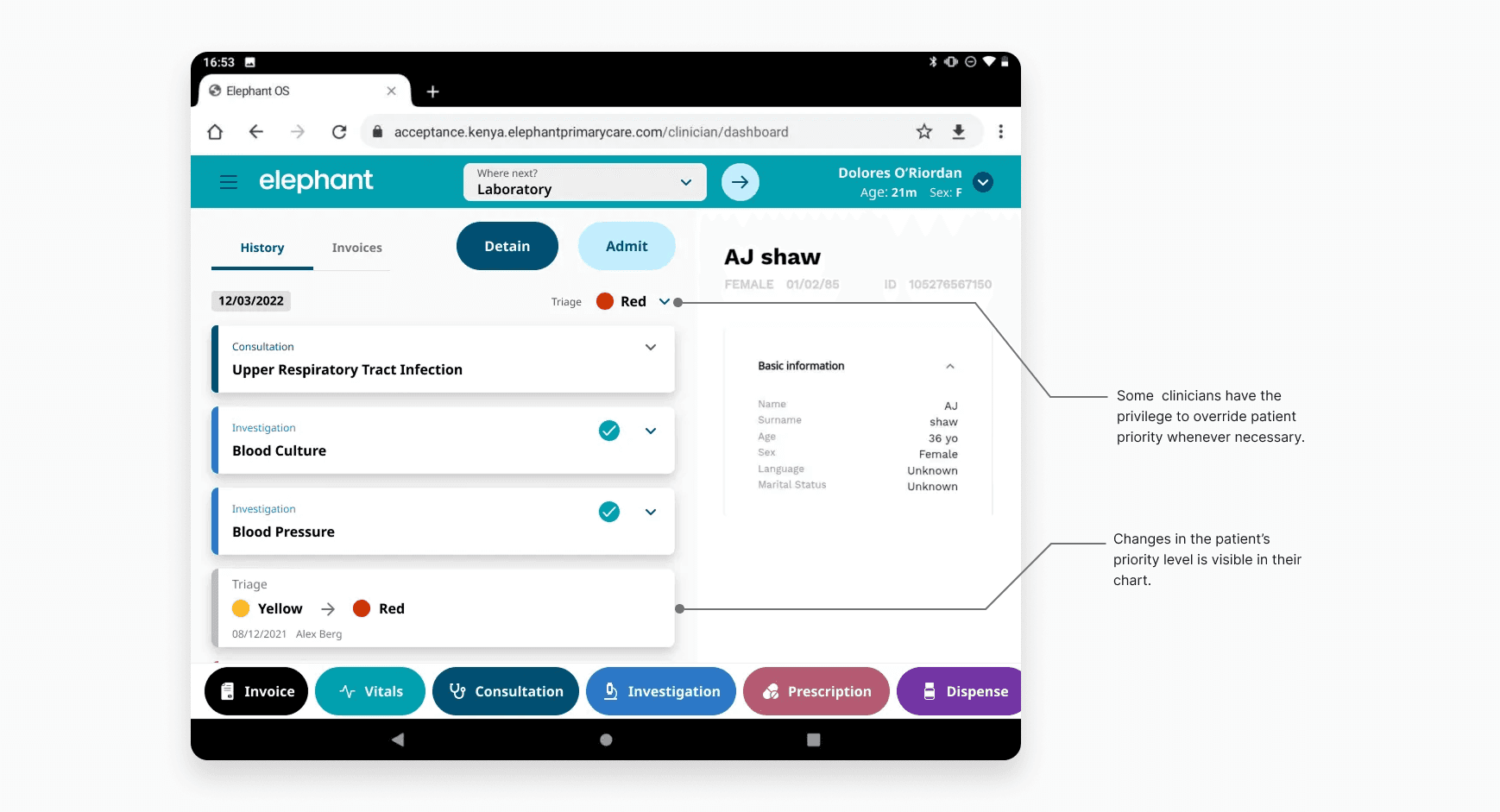
Making the patient triage sensitive to real-time care events so a patient’s priority changes automatically with any change in their condition, even when on admission.
Strategic Decisions